

Figure 1: Ligature Marks
It's a Sunday morning, and my friend and I are sitting in a conference room learning about the physical exam findings suggestive of torture. The lights in the auditorium dim, and an attorney walks to the podium. She explains the steps of the asylum process, who might be eligible, how long it takes, and how few applications are accepted. How they need doctors like us to provide an objective, scientific voice to contrast those of the bleeding-heart immigration lawyers. Then a physician takes her place, ostensibly to teach us how to perform the medical screening exam that will be used as evidence in an asylum case. Emotionless, he clicks through slides of the various methods used as torture -- waterboarding, finger crushing, electrocution, rape, etc -- and the markings they leave on the body. All the ways in which to crush a human spirit. The more evidence we find, the stronger the case. The attorney smiles encouragingly. I avert my gaze.

Figure 2: Metacarpal fractures consistent with trauma, my daughter's bow
When I see these photos, all I can think of is my daughter. So helpless at 9 months of age. What I wouldn't do to protect her.

Figure 3: My family on Halloween, dressed up like giraffes
While an applicant waits for their case to be evaluated, they are able to stay in the US. Given a permit to work. Granted a small space to breathe. During the slide about how to document scars, my friend leans over to ask me, "but how can I be sure that these skin markings are from torture? What if they are from childhood injuries? If I judge incorrectly, and that person is granted asylum, does that mean it is denied to someone else?" The weight of that decision feels too heavy. I decide I will pretend it doesn't exist.

Figure 4: The Dermal Markings of Cigarette Burns Over Time
At lunch, we sit at a table with four young strangers, eagerly saying how they want to help. I learn that they are all medical students. Fitting. They haven't yet lost their eager optimism, forgotten the reasons they went into medicine. My friend and I may be the only attendings in the audience. Where are the rest? The ones who arguably have more authority, more experience, more to offer? Where are they?
I can imagine, as my friend and I are about to sneak out of the conference early in order to join them. They are probably playing baseball with their kids, or out to brunch with friends, the tension from the hospital workplace dramas slowly dissipating from their taut shoulders. It's 75 degrees and sunny out. Now that we have finished the slog of medical school and residency, we no longer have to work eighty hours a week. Finally, we don't have to sacrifice quite so much. Now is the time to make up for all the years lost. The balance the only way to survive the years of practice that stretch ahead. The enjoyment of health the only way to live in the face of never-ending suffering and illness.

Figure 5: Chapter 3, Section 4: Medical Evidence [of torture]
104. In formulating a clinical impression for the purposes of reporting physical and psychological evidence of torture, there are six important questions to ask:
(a): Are the physical and psychological findings consistent with the alleged report of torture?
(b): What physical conditions contribute to the clinical picture?
(c): Are the psychological findings expected or typical reactions to extreme stress within the culture and social context of the individual?
(d): Given the fluctuating course of trauma-related mental disorders over time, what is the time-frame in relation to the torture events? Where in the course of recovery is the individual?
(e): What other stressful factors are affecting the individual (e.g. ongoing persecution, forced migration, exile, loss of family and social role, etc.)? What impact do these issues have on the victim?
(f): Does the clinical picture suggest a false allegation of torture?
~~~

Figure 6: The Eloy Detention Center is a private prison located in Eloy, Pinal County, Arizona, owned and operated by CoreCivic, formerly the Corrections Corporation of America, under contract with the U.S. Immigration and Customs Enforcement
A few weeks later, I am fidgeting outside the 1st locked door at the large ICE detention center in Eloy. Fencing laced with barbed wire stretches out in all directions around me. The air is dry and smells like cow shit. The horizon is the hazy tan color of pollution. Although I can't see the guards, they can see us. We hear a buzz, followed by the mechanical clank of the metal door unlocking. We walk through a corridor to another door. We again wait. The first door locks behind us as the one in front opens.
The guards are in the khaki green uniforms, and are annoyed that my friend has forgotten our official documents granting us clearance. They check a binder sitting on the counter, but our verification is nowhere to be found. Phones are not allowed past the security checkpoint, so she has to go back out to the car, retrieve her phone, bring it back inside, pull up the email, show it to the guard, and then return it to the car. There is some confusion as to whether or not we are at the right facility, it is possible that our client has been moved to another detention center in the area. There are several out here. After a few calls via her radio, the guard determines that our client is, in fact, here, but nobody knew he was supposed to have been brought from his cell in time for his 9 am appointment. We are filed through the metal detector, our legs are patted down, and then wait some more, this time in an internal waiting room between the security checkpoint and another locked door.
I scan the waiting room. There are several benches, much like church pews, stacked in horizontal rows. Most of the other visitors are families, everyone wearing nice dresses, polished shoes, and pressed slacks. A young mother feeds a bottle to a baby swaddled in blankets. A small TV is hanging in the corner. It's playing a silly kids' movie featuring colorful, animated snails with exaggerated facial expressions.

Figure 7:My stethoscope over sample medical documentation of trauma
The door under the TV swings open, and a guard calls our names. We follow him into another room with tables where detainees can meet their guests, and then into a small cell where our client, who we've never met before, is standing. He has a small frame and his eyes remain focused on the floor. He is biting the inside of his lip. Usually we perform these exams in the clinic, my friend tells the guard. Can we be moved there? We have to examine him and this isn't the best location. Also, we brought this gown for him to change into. The guard sighs.
Well that will take more time. We may not be able to fulfill that request.
We understand, but if you can, we'd appreciate it.
The guard leaves. The three of us remain standing it the small room. It is freezing, I wish I had brought a jacket. Our client is wearing a worn uniform, it's cotton thinning. It looks the same as what the prisoners wear when they are brought to my hospital. I have to remind myself that our client is not a prisoner, that we are not in a prison -- our client is seeking asylum under international law.
128. Interviews with people who are still in custody, and possibly even in the hands of the perpetrators of torture obviously will be very different from interviews in the privacy and security of an outside and safe medical facility. The importance of obtaining the person's trust in such situations cannot be stressed enough. However, it is even more important not to, even unwittingly, betray that trust. All precautions should be taken so that detainees do not place themselves in danger.
Five minutes later, and the guard returns. We follow him down locked hallways until we are brought to the clinic. Immediately, the air feels a little lighter. The nurses and doctor wave at us as we walk past their counter. We are brought to a room that feels just like any other clinic room, with chairs and a medical examining table. No guards are within sight. But still, the chill remains. I cross my legs and wrap my arms around my elbows, trying to conserve warmth. For the next two hours, we struggle to piece together a cohesive narrative about the man sitting in front of us. He rarely makes eye contact, talks in a hushed voice, and slurs his words. He was tortured when he was a child, and dropped out of school immediately thereafter. His memories about the incident and his life during that time are extremely vague. They also don't move in a linear, chronologic fashion. This is diagnostic of childhood trauma, but how can I convey that to a judge if I don't have the facts to back it up? Will the judge assume that a lack of details is instead diagnostic of a fabricated narrative?
He also shies away from our attempts to label him with diagnoses of illness, such as PTSD, anxiety, and alcohol use disorder. When I rattle off a list of symptoms whose presence are considered diagnostic, he denies all of them. I imagine that he wants to show us that he isa a survivor, not a victim. That he has overcome. That his scars have been erased. Invisible to the probing eye.

Figure 8: Child Dissociative Checklist juxtaposed against a fisher-price cross
Below is a list of behaviors that describe children. For each item that describes your child now or within the past 12 months, please circle 2 if the item is very true of your child. Circle 1 if the item is somewhat or sometimes true of your child. If the item is not true of your child, circle 0.
0 1 2 1. Child does not remember or denies traumatic or painful experiences that are known to have occurred
0 1 2 2. Child goes into a a daze or trance like-state at times or often appears "spaced-out." Teachers may report that he or she "daydreams" frequently in school
0 1 2 3. Child shows rapid changes in personality. He or she may go from being shy to being outgoing, from feminine to masculine, from timid to aggressive.
0 1 2 4. Child is unusually forgetful or confused about things that he or she should know, e.g. may forget the names of friends, teachers, or other important people, loses possessions or gets easily lost.
0 1 2 5. Child has a very poor sense of time. He or she loses track of time, may think that it is morning when it is actually afternoon, gets confused about what day it is, or becomes confused about when something has happened.
0 1 2 6. Child shows marked day-to-day or even hour-to-hour variations in his or her skills, knowledge, food preferences, athletic abilities, e.g. changes in handwriting, memory for previously learned information such as multiplication tables, spelling, use of tools or artistic ability.
0 1 2 7. Child shows rapid regressions in age-level behavior, e.g. a twelve-year-old starts to use baby-talk, sucks thumb or draws like a four-year old
0 1 2 8. Child has a difficult time learning from experience, e.g. explanations, normal discipline or punishment do not change his or her behavior.
0 1 2 9. Child continues to lie or deny misbehavior even when the evidence is obvious.

Figure 9: Review of Torture Methods
143. After eliciting a detailed narrative account of events, it is advisable to review other possible torture methods....Questioning about specific forms of torture is helpful with:
(a) Psychological symptoms cloud recollections
(c) in the case of possible organic brain damage
144. The distinction between physical and psychological methods is artificial.... the entire clinical picture produced by torture is much more than the simple sum of lesions produced by methods on a list.
H. Risk of re-traumatization of the interviewee [is very likely]
~~~

Figure 10: Vials of influenza vaccine upon my daughter's block
I arrive at Casa Alitas just in time for the arrival of twenty asylees just released from ICE custody. It's my first time volunteering with this NGO, so I wander over to a man sitting behind a desk with a sign-in sheet. There is another young man also checking in, a medical student here for the first time. The front-desk-man seems unphased by new volunteers just showing up, and gestures towards the opposite end of the large building, "Find Barb, she'll orient you."
She shows us a form that we are to use when conducting our medical interviews."Usually we also offer flu vaccines, but we don't have anyone available to give them today."
I spend the next hour administering about twenty vaccines to families from Ecuador, Guatemala, and El Salvador. The atmosphere in the room is jovial, a sharp contrast to the mood when I give injections to kids in my hospital. What have they endured to make this seem like a pleasant experience? One at a time, kids march up to my table, boldly rolling up their sleeve and offering the flesh of their arms. They squeeze their eyes shut as I pierce their skin, and then laugh when it is over, bragging to their siblings how it didn't even hurt. Their parents laugh. Everyone gets candy. We hand them a packet, Bienvenidos a America.
Although most everyone I meet that day is their with their family members, there are two women who are alone. They appear to be in their second trimester of pregnancy. I remember how vulnerable I felt while pregnant, every day a new opportunity to cause harm to my unborn child or my bloated, unsteady body.
~~~
Things I hear from other volunteers and healthcare providers:
Usually, when they arrive here, they complain that their stomachs hurt because all they are given to eat in custody are tortillas and ritz crackers. They are usually in detention for several days.
Even though they aren't supposed to be separating families anymore, a woman was separated from her 14-year-old brother because she was not his parent. He was classified as an unaccompanied minor.
We responded to a 911 call for a kid with abdominal pain at a detention facility. There were multiple cells full of just children of various ages. Each cell seemed to have an older kid covered with little ones clambering over them.
When we transfer pediatric patients in an ambulance from our rural hospital to the regional center with pediatric specialists, we often send them without their parents, as CBP will physically remove undocumented parents from ambulances as they pass through the immigration checkpoint. So we have these little kids, scared, undergoing surgeries in a strange place and without the comfort of their families. Can you imagine sending your child alone? [I imagine my baby naked in a cold operating room, hands in blue gloves holding down her flailing arms and legs, a mask pumping anesthetic gases held firm over her face, muffling her cries]
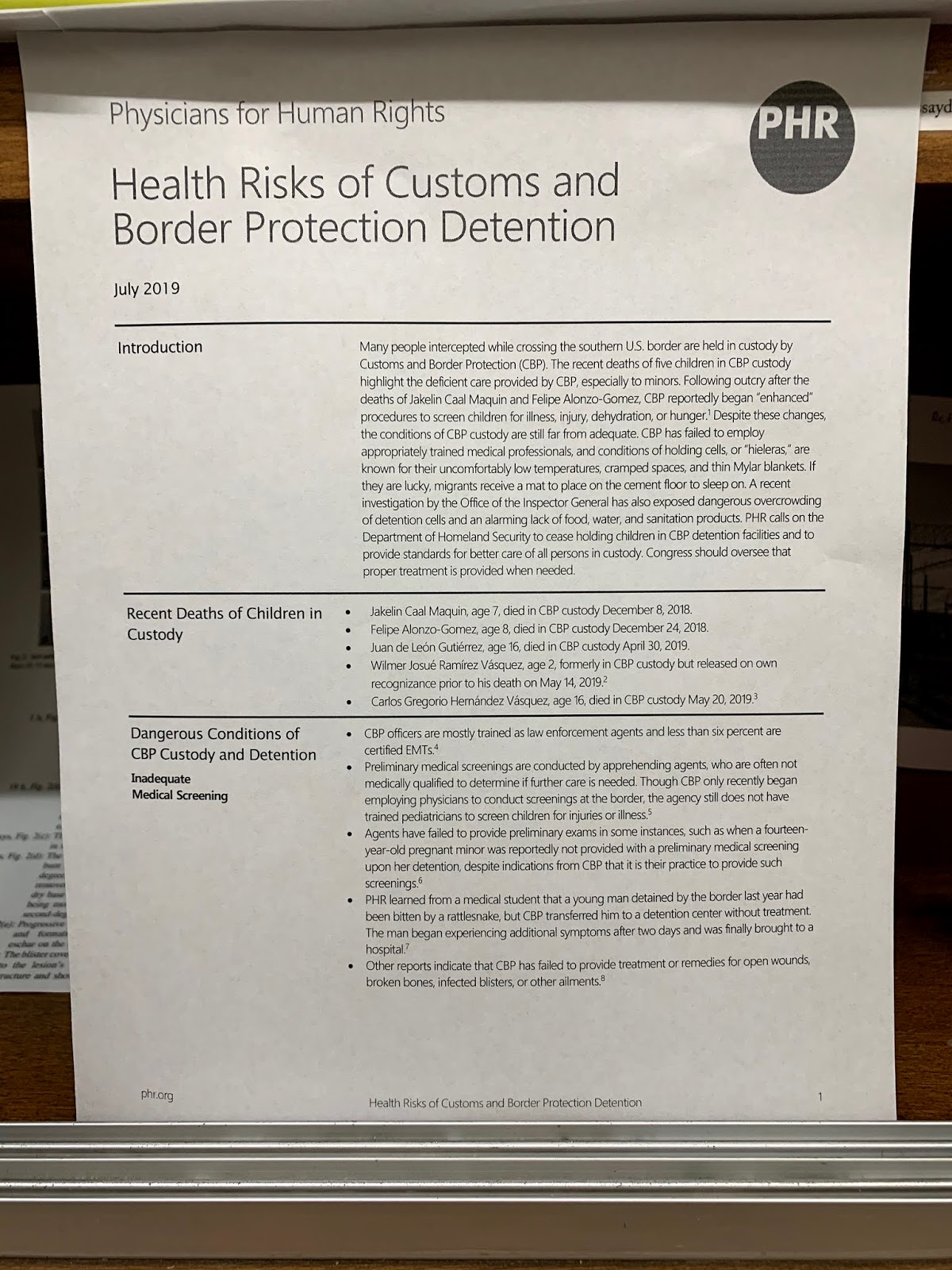
Figure 11: Health Risks of Customs and Border Protection Detention
Recent deaths of children in custody:
- Jaelin Caal Maquin, age 7
- Felipe Alonzo-Gomez, age 8
- Juan de León Gutiérrez, age 16
- Wilmer Josué Ramírez Vásquez, age 2
- Carlos Gregorio Hernández Vásquez, age 16
From the Istanbul Protocol:
54. Health professionals also have a duty to support colleagues who speak out against human rights violations. Failure to do so risks not only an infringement of patient rights and a contravention of the declarations listed above but also brings the health professions into disrepute. Tarnishing the honour of the profession is considered to be serious professional misconduct. The World Medical Association's resolution on human rights calls on all national medical associations to review the human rights situations in their own countries and ensure that doctors do not conceal evidence of abuse even where they fear reprisal...It calls upon individual doctors to speak out against maltreatment and urges national and international medical organizations to support doctors who resist such pressure.
~~~
From the Joint Letter to Deputy Director Homan Regarding ICE Procedures for Pregnant Women, written by AAP, ACOG, and AAFP:
It has been documented that while in immigration detention facilities, pregnant women and adolescents experience poor access to medical care, and are highly vulnerable to sexual assault. Although standards were published by ICE to improve women’s access to reproductive health care, including prenatal care, facility adherence to these standards is unknown. In 2016, the Department of Homeland Security’s (DHS) Advisory Committee on Family Residential Centers recommended that barring extraordinary circumstances, no pregnant woman or her children should be detained in a family residential center.
All pregnant women and adolescents held in federal custody, regardless of immigration status, should have access to adequate, timely, evidence-based, and comprehensive health care. Pregnant immigrant women and adolescents should have access to high levels of care, care that is not available in these facilities. The conditions in DHS facilities are not appropriate for pregnant women or children. A growing body of evidence suggests that maternal psychological state can negatively affect fetal and child development, and practices like shackling during pregnancy, which have been reportedly used at ICE facilities, have serious negative physical and mental health impacts on pregnant women.
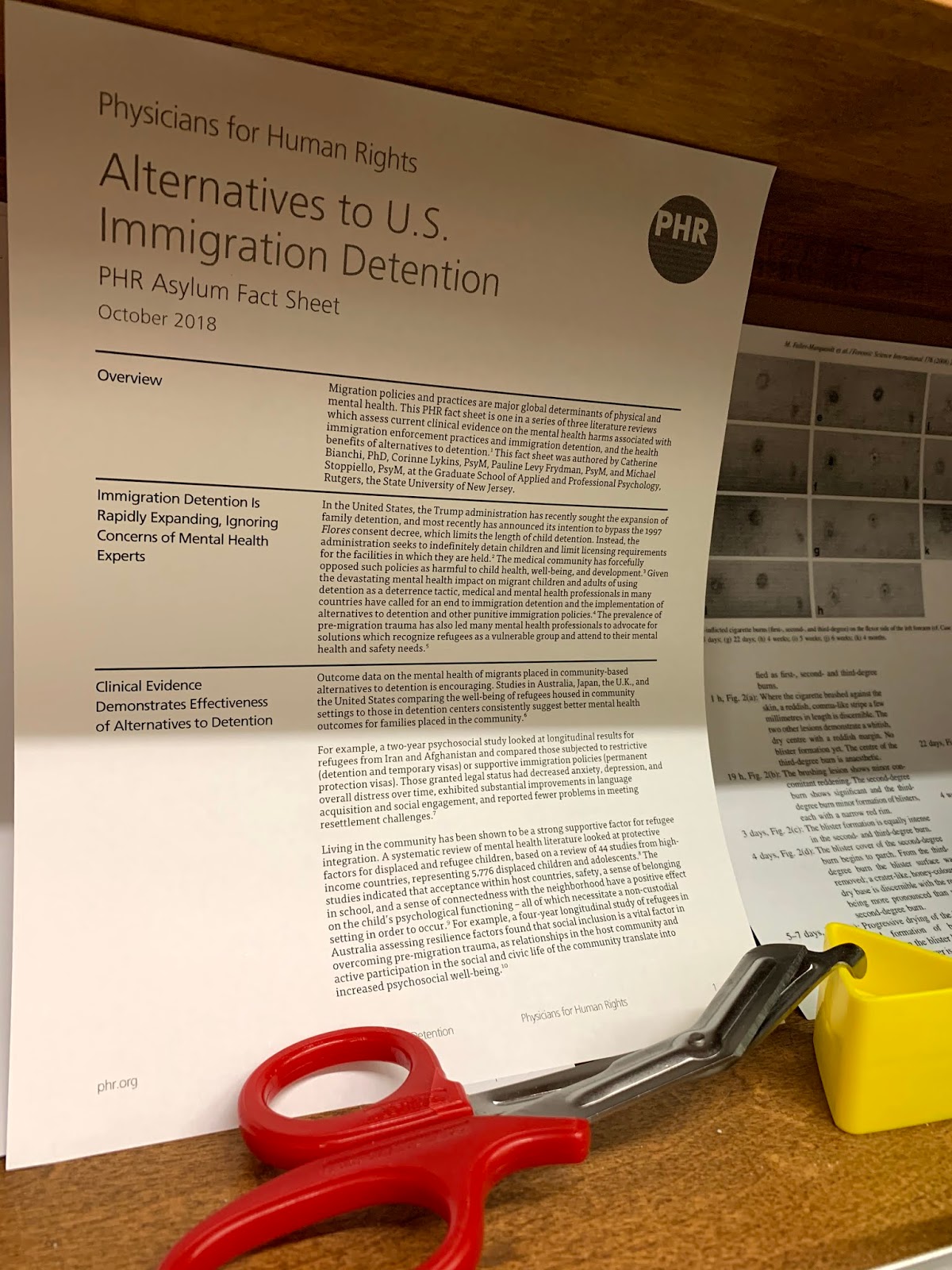
Figure 12: Alternatives to U.S. Immigration Detention, trauma shears, and my daughter's fisher-price triangle
Medical Decision Making:
Innocent people are tortured. They seek asylum in the US. We treat them like prisoners and harm them further, inflicting trauma whose effects will persist for generations. It doesn't have to be this way.

Figure 13: The Sum of its Parts
No comments:
Post a Comment